


Keyword Search
Treatment for Early Stage Endometrioid Adenocarcinoma of the Corpus at Gleneagles Hospital Hong Kong (GHK) – The GHK Experience
Overview of carcinoma of the corpus
Carcinoma of the Corpus is the commonest gynaecological cancer in Hong Kong. According to the latest figures from the Hong Kong Cancer Registry (www3.ha.org.hk/cancereg/), it ranks 4th amongst the commonest female cancers. Fortunately, most women with carcinoma of the corpus present early with postmenopausal bleeding. Therefore 3 of 4 patients with carcinoma of the corpus are at the earliest Stage 1 at presentation, where the cure rate is very high in excess of 80%. It is important to note that Pap smears may be normal in patients with carcinoma of the corpus.
Women who present with postmenopausal bleeding to a gynaecologist will have an ultrasound done in addition to a gynaecological examination. Most women who present with postmenopausal bleeding do not have cancer, and may have a normal ultrasound finding. However, a minority may have a thickened endometrial lining of the uterus. In a normal postmenopausal woman, the endometrial thickness should be 5 mm or less. Anything more than this may be indicative of hyperplasia, a type of which is pre-cancerous, or cancer. The gynaecologist will try to obtain a histological sample from the endometrial lining using an office procedure called endometrial aspirate. This method is more than 90% accurate in diagnosing carcinoma of the corpus. Alternatively, the gynaecologist may arrange for a diagnostic hysteroscopy and curettage to obtain a histological diagnosis.
One of 4 women with carcinoma of the corpus presents with abnormal menstrual bleeding before menopause. While most patients with abnormal menstrual bleeding after the age of 40 have a diagnosis of dysfunctional uterine bleeding due to hormonal imbalance in the few years before the menopause, carcinoma of the corpus must be considered as one of the possible diagnosis especially if she does not respond to hormonal treatment.
After the diagnosis of carcinoma of the corpus is confirmed by histological examination, the patient will usually be referred to a gynaecological oncologist, who can further evaluate the
patient to stratify her into the appropriate risk status for definitive surgical management.
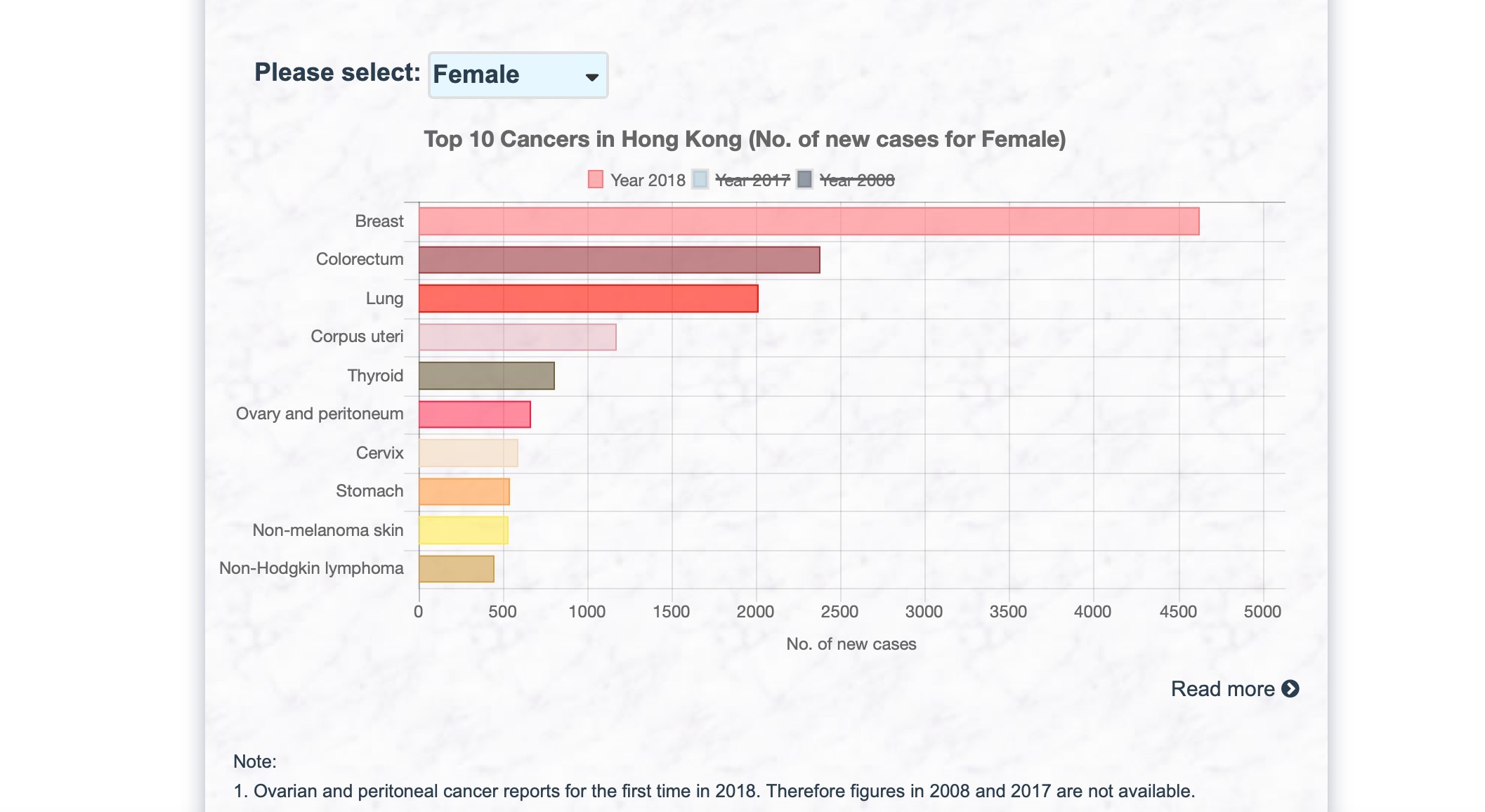
Hong Kong Cancer Registry, Hospital Authority (www3.ha.org.hk/cancereg)
In Gleneagles Hospital Hong Kong (GHK), the Gynaecological Oncologist is supported by a multi-disciplinary team consisting of gynaecological oncologists, clinical oncologists, surgical oncologists, medical oncologists, radiologists and pathologists. This multi-disciplinary team of doctors constitute the Gynaecological Oncology Tumour Board. Since the inception of the hospital, the Gynaecological Oncology Tumour Board has met regularly every month. This meeting is open to all doctors interested in the management of gynaecological cancers.
The Gynaecological Oncology Tumour Board meets regularly to consider the latest evidence-based treatment for patients with gynaecological cancers, to see which of these treatments and procedures can be safely and effectively applied to patients with gynaecological cancers at GHK. The speed of advance in cancer care is such that the team needs to be up to date with the latest research, and the full arsenal of available surgery, radiotherapy, chemotherapy, targeted therapy and other proven treatments can be considered for patients at GHK.
The Gynaecological Oncology Tumour Board also discusses all patients with gynaecological cancers operated on in GHK, to ensure that patients are receiving the most appropriate care. This also serves as an audit and check on the treatment provided by all doctors accredited to perform gynaecological cancer procedures in GHK. To our knowledge, it is the only private hospital in Hong Kong to have a dedicated, regular meeting of the Gynaecological Oncology Tumour Board for this purpose.
The multi-disciplinary nature of the Gynaecological Oncology Tumour Board ensures that the combined experience of the members of the team are utilised in the management of every patient with gynaecological cancer in GHK. The open and frank audit of the management of patients ensures quality assurance for patients at GHK. It is a key tenet of GHK’s partnership with The University of Hong Kong to build, promote and implement strong clinical governance at GHK.
Since the advent of the Gynaecological Oncology Tumour Board, other surgical disciplines at GHK have also started regular tumour board meeting for their respective specialties at GHK as the benefits and advantages of a multi-disciplinary team approach for the management of complex cancer cases are seen.
The gynaecological oncologist upon seeing the patient for the first time will take a thorough history and perform a physical examination including a gynaecological and ultrasound examination. The histology report and MRI report (if available) will be reviewed. If an MRI is not available, an MRI of the abdomen and pelvis will be arranged.
These are the questions that need to be answered after the consultation with the gynaecological oncologist:
- What histological cell type is the cancer? The commonest cell type is endometrioid adenocarcinoma which is the focus of this article.
- What is the grade of the cancer (Grade 1, 2 or 3)?
Grade 1 (well-differentiated ) or Grade 2(moderately differentiated) are considered low grade cancers while Grade 3(poorly differentiated) cancers are considered high grade cancers with a higher chance of spread of the cancer. - What is the stage of the cancer – is there any evidence of spread of cancer based on the available evidence?
Fortunately, 75% of patients with endometrioid adenocarcinoma are Stage 1 or Stage 2 (occult) at presentation. - Is the patient suitable for surgery and if so is she suitable for a minimally invasive (laparoscopic) hysterectomy?
Based on this assessment, the patient will be stratified into either low risk or high risk for lymphatic spread of cancer.
A patient classified as low risk for lymphatic spread of cancer with no contraindication for surgery will be counselled for a laparoscopic hysterectomy bilateral salpingo-ophorectomy (removal of her uterus and both tubes and ovaries). If laparoscopy is not advisable, the gynaecological oncologist may advise an open surgery to remove the uterus and both tubes and ovaries.
If the patient is classified as high risk for lymphatic spread of disease (Table 1), in addition to removal of the uterus, tubes and ovaries, a staging procedure involving removal of pelvic with or without para-aortic lymph nodes will be done to look for lymphatic spread of disease which will affect the final staging as well as the necessity for adjuvant treatment such as radiotherapy.
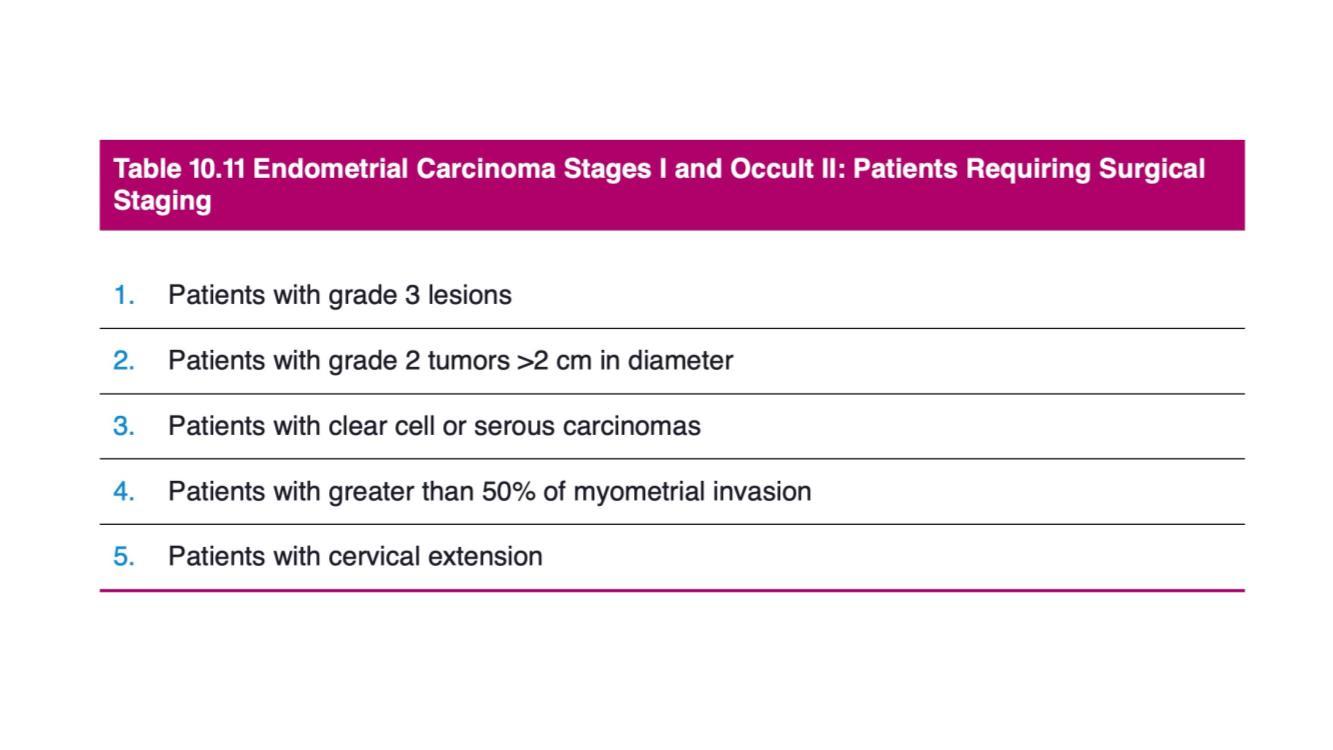
Table 1: Table from Chapter 10, Berek & Hacker’s Gynecologic Oncology, 7th Edition, Wolters Kluwer
The standard surgical treatment for early stage low risk carcinoma of the corpus is a laparoscopic hysterectomy bilateral salpingo-ophorectomy. Laparoscopy (minimally invasive surgery) rather than laparotomy (open surgery) is now the established method of surgery for early stage carcinoma of the corpus, with an equivalent survival outcome but associated with faster recovery, reduced hospital stay and adverse outcomes, and better quality of life1,2,3,4.
For early stage high risk carcinoma of the corpus, in addition to removal of the uterus, both tubes and ovaries; pelvic lymphadenectomy with or without para-aortic lymphadenectomy will also be done for a thorough surgical staging. This is necessary so that a tailored postoperative adjuvant treatment can be recommended based on the final histology results.
The extent of surgery, and the approach to surgery is in a constant state of evolution as gynaecological oncologists strive to achieve the best results for their patients with minimal trauma. Therefore, in GHK, we have been doing Single Incision Laparoscopic Surgery (SILS) or Vaginal Natural Orifice Transluminal Surgery (vNOTES) for suitable patients with early stage low risk carcinoma of the corpus. In SILS, patients have only a single wound at the umbilicus. In vNOTES, the whole procedure including laparoscopy is done vaginally and there are no visible abdominal wounds.
In partnership with The University of Hong Kong (HKU) and other leading institutions, GHK is also actively involved in research on new techniques and instruments which minimise trauma for patients without impacting on survival. The safety of patients is our first priority in all these ongoing research and improvement.
The results after staging surgery are a guide to whether a patient will require any adjuvant treatment to further decrease the chance of recurrence. Any additional treatment has potential side-effects. It is necessary to decide which patients will benefit from additional treatment or which patients need observation only without additional treatment. There are several guidelines and these guidelines will also change as new information such as molecular profiling of tumours become available in the future. For now in GHK, the ESMO-ESGO-ESTRO (2016) guideline is used. Based on this and individual patient factors, the gynaecological oncologist will decide which additional treatment, if any, will benefit the patient. In this regard, the Gynaecological Oncology Tumour Board, with the combined experience and input of its multi-disciplinary members, will also come to a consensus opinion based on a discussion of the individual patient factors and histology.
Carcinoma of the Corpus is the commonest gynaecological malignancy. Fortunately, most patients are diagnosed at an early stage where the cure rate is very high. It is the responsibility of the gynaecological oncologist to choose the most appropriate surgery for the patient based on pre-operative risk factors. After the surgery and based on the post-operative findings and histology, the gynaecological oncologist chooses the most appropriate post-surgery options, which, depending on the postoperative risk stratification may range from observation only, vaginal brachytherapy to external beam radiotherapy with or without chemotherapy. The full range of adjuvant therapies are currently provided at GHK.
At GHK, we are committed to the latest evidenced-based management. However, we recognise that every woman is an individual, and we seek to apply those guidelines to individual women based on their unique circumstances. In this quest, the gynaecological oncologist benefits from the combined expertise and experience of the multi-disciplinary Gynaecological Oncology Tumour Board to help in decision making.
At GHK, we are actively involved in cutting edge research in collaboration with HKU and other leading international institutions utilising IDEAL guidelines (https://www.ideal-collaboration.net) to research the latest robotic endoscopes and instrumentations6. We seek to obtain the best and most cost-effective instruments available for appropriate minimally invasive surgery for our patients without compromising their safety and survival, taking into consideration the financial implications of these new technologies. In addition to benefits for patients, at GHK we are also seeking surgical technologies that improve ergonomics and the operative environment for our gynaecological surgeons to enable them to perform at their optimal best for patients without compromising their own health and safety.
It is this commitment to our patients that prompts us to continue to investigate such emerging advances as molecular profiling of carcinoma of the corpus for risk stratification, and sentinel lymph node mapping in place of complete lymphadenectomy in at risk patients.
At GHK, our multidisciplinary team in Gynaecological Oncology are committed to offering the best evidence-based treatment for our women with carcinoma of the corpus. Our priority is to ensure that our patients receive the safest and most cost-effective care. Working together and taking full advantage of the combined experiences of our multidisciplinary team members, we are committed to providing the most appropriate and innovative care for our patients.
Patient’s condition
Mrs. Wong, a 60-year-old mother of two and grandmother of one, complained of postmenopausal bleeding. She had her menopause eight years ago at 52 years old. She has regular yearly gynaecological check-up with her gynaecologist of many years, and Pap smears and pelvic ultrasound examinations have been normal. She had a normal gynaecological check-up just six months ago. She noticed blood stains on her panties for two days. She was otherwise healthy and had no other complaints. Apart from vitamin supplements, she was on no other regular medication or supplements.
She decided to consult with her regular gynaecologist who proceeded to a gynaecological examination and pelvic ultrasound examination. Ultrasound showed a thickened endometrial lining to 1.2 cm ( a normal postmenopausal lining should be less than 5 mm thick ). Her gynaecologist proceeded to do an endometrial aspirate in the office and sent it for histology.
Three days later she received a call to see her gynaecologist who explained that the endometrial aspirate showed that she had Endometroid Adenocarcinoma of the Corpus Grade 2. She was then referred to a Gynaecological Oncologist for further management.
Examination and diagnosis
Mrs. Wong was seen by a gynaecological oncologist. Her histological report was reviewed. A transvaginal ultrasound examination showed a normal sized uterus. The endometrial thickness was 1.2 cm. There was minimal spread of tumour into the muscle of the uterus (myometrial invasion). Both ovaries were seen and were normal size. A provisional diagnosis of clinical Stage 1aG2 endometrioid adenocarcinoma was made. She was booked to have an outpatient MRI abdomen and pelvis for pre-operative staging and risk stratification.
Mrs. Wong was seen with the results of the MRI which showed a 1.2 x 2.5 cm endometrial tumour invading to less than 50% of the muscle of the uterus (myometrium). There was no evidence of spread of tumour outside the uterus. She was categorised to be at higher risk for lymphatic spread of disease because of the Grade 2 histology and largest tumour diameter of more than 2 cm. She was recommended to have a Total Laparoscopic Hysterectomy Bilateral Salpingo-Ophorectomy and Bilateral Pelvic Lymphadenectomy (removal of her uterus, tubes, ovaries and lymph nodes in the pelvis using minimally invasive surgery). The surgical procedure and risks were explained to her and a consent for surgery was taken. A fee advisory was also obtained for her with an estimation of the total hospital costs of the surgery in GHK.
Treatment journey
Mrs. Wong was admitted to GHK at 8 pm the evening before her surgery which was scheduled for 8 am the next morning. Pre-operative blood tests, chest x-ray and ECG were done. The nurses then prepared her for surgery by giving her an enema to clear her bowels, and she was asked to fast from solid food after 12 midnight. However, she could continue to have clear fluids until 6 am, two hours before her surgery. Any further questions she had regarding the surgery were answered by the medical staff. Her anaesthetist also saw her before the surgery to explain about the general anaesthesia and post-surgery pain control and risks as well as to obtain a consent for anaesthesia.
The next morning, she had a total laparoscopic hysterectomy bilateral salpingo-ophorectomy and bilateral pelvic lymphadenectomy which was done successfully with minimal blood loss. She made an uneventful post-surgery recovery and was taking food orally the same evening of the surgery. She was discharged from hospital once she was fully mobile, eating normally and was mentally prepared to go home. She was given an appointment to see her gynaecological oncologist in one week’s time to check her wound as well as to review the final histology reports.
The histology of Mrs. Wong showed a Stage Ia Grade 2 Endometroid Adenocarcinoma of the Corpus. The surgical margins were clear. There was no metastasis to the pelvic lymph nodes. However, there was substantial lymphovascular-space invasion of tumour cells. According to the ESMO-ESGO-ESTRO (2016) guideline5, she should be offered vaginal brachytherapy (radiation to the vaginal vault) to decrease the chance of local recurrence. Her case was also discussed at the monthly Gynaecological Oncology Tumour Board, and the consensus opinion was to offer her the option of vaginal brachytherapy.
Mrs. Wong was seen one week after the surgery. Her abdominal wounds were well-healed. She was then seen again one month after the surgery and her vaginal wound was well-healed. Her histology results were discussed with her, and adjuvant vaginal brachytherapy was offered. She was referred to a Clinical Oncologist for an expert opinion and discussion regarding adjuvant radiotherapy.
Mrs. Wong received vaginal brachytherapy 6 weeks after her surgery in GHK which consisted of 4 sessions over two weeks. She tolerated the treatment well. She has now completed all treatment and will be seen once every 3 months for the first two years after completion of treatment, then once every 6 months from the third to the fifth year and then yearly thereafter. At each visit, she will have a gynaecological examination and a vault smear.
- Janda M, Gebski V, Brand A, Hogg R, Jobling TW, Land R, Manolitsas T, McCartney A, Nascimento M, Neesham D, Nicklin JL, Oehler MK, Otton G,
Perrin L, Salfinger S, Hammond I, Leung Y, Walsh T, Sykes P, Ngan H,
Garrett A, Laney M, Ng TY, Tam KF, Chan K, Wrded CDH, Pather S, Simcock B, Farrell R, Obermair A. (2010) Quality of Life after total laparoscopic hysterectomy versus total abdominal hysterectomy for stage I endometrial cancer (LACE): a randomized trial. Lancet Oncol 11(8):772-80
- Andreas Obermair, Monika Janda, Jannah Baker, Srinivas KondalsamyChennakesavan, Alison Brand, Russell Hogg, Thomas W Jobling, Russell
Land, Tom Manolitsas, Marcelo Nascimento, Deborah Neesham, James L
Nicklin, Martin K Oehler, Geoff Otton, Lewis Perrin, Stuart Salfinger, Ian
Hammond, Yee Leung, Peter Sykes, Hextan Ngan, Andrea Garrett, Michael Laney, Tong Yow Ng, Karfai Tam, Karen Chan, David H Wrede, Selvan Pather, Bryony Simcock, Rhonda Farrell, Gregory Robertson, Graeme Walker,Anthony McCartney, Val Gebski. (2012) Improved surgical safety after laparoscopic compared to open surgery for apparent early stage endometrial cancer: results from a randomized controlled trial. Eur J Cancer 48(8):1147-53
Srinivas Kondalsamy-Chennakesavan, Monika Janda, Val Gebski, Jannah Baker, Alison Brand, Russell Hogg, Thomas W Jobling, Russell Land, Tom
Manolitsas, Marcelo Nascimento, Deborah Neesham, James L Nicklin, Martin K Oehler, Geoff Otton, Lewis Perrin, Stuart Salfinger, Ian Hammond, Y carcinoma of the corpus ee
Leung, Peter Sykes, Hextan Ngan, Andrea Garrett, Michael Laney, Tong Yow Ng, Karfai Tam, Karen Chan, David H Wrede, Selvan Pather, Bryony Simcock, Rhonda Farrell, Gregory Robertson, Graeme Walker, Anthony McCartney, Andreas Obermair. (2012) Risk factors to predict the incidence of surgical adverse events following open or laparoscopic surgery for apparent early stage endometrial cancer: results from a randomized controlled trial. Eur J Cancer 48(14):2155-62Monika Janda, PhD; Val Gebski, MStat; Lucy C. Davies, MSc; Peta Forder, MBiost; Alison Brand, FRANZCOG; Russell Hogg, FRANZCOG;
Thomas W. Jobling, FRANZCOG; Russell Land, FRANZCOG; Tom Manolitsas, FRANZCOG; Marcelo Nascimento, FRANZCOG;
Deborah Neesham, FRANZCOG; James L. Nicklin, FRANZCOG; Martin K. Oehler, FRANZCOG; Geoff Otton, FRANZCOG; Lewis Perrin, FRANZCOG; Stuart Salfinger, FRANZCOG; Ian Hammond, FRANZCOG; Yee Leung, FRANZCOG; Peter Sykes, FRANZCOG; Hextan Ngan, MD;
Andrea Garrett, FRANZCOG; Michael Laney, FRANZCOG; Tong Yow Ng, MD; Karfai Tam, MB, BS; Karen Chan, MB, BChir; C. David Wrede, MD; Selvan Pather, FRANZCOG; Bryony Simcock, FRANZCOG; Rhonda Farrell, FRANZCOG; Gregory Robertson, FRANZCOG; Graeme Walker, MD; Nigel R. Armfield, PhD; Nick Graves, PhD; Anthony J. McCartney, FRANZCOG; Andreas Obermair, MD, FRANZCOG(2017) Effect of Total Laparoscopic Hysterectomy vs Total Abdominal Hysterectomy on Disease-Free Survival Among Women With Stage I Endometrial Cancer: A Randomized Clinical Trial JAMA 2017, 317(12): 1224Colombo N, Creutzberg C, Amant F, et al. ESMO-ESGO-ESTRO consensus conference on endometrial cancer: diagnosis, treatment and follow-up. Int J Gynecol Cancer 2016;26:2–30.
McCulloch P, Altman DG, Campbell WB, et al. No surgical innovation without evaluation: the IDEAL recommendations. Lancet. 2009 Sep 26;374(9695):1105-12.
Download or print “Treatment for Early Stage Endometrioid Adenocarcinoma of the Corpus at Gleneagles Hospital Hong Kong (GHK) – The GHK Experience”

Related services
- Gynaecological Oncology Centre
- Haematology & Oncology Clinic
- Obstetrics & Gynaecology Clinic
- Peritoneal Malignancy Treatment Centre
- Radiotherapy and Oncology Centre